Fill in Your First Report Of Injury Florida Form
Fill in Your First Report Of Injury Florida Form
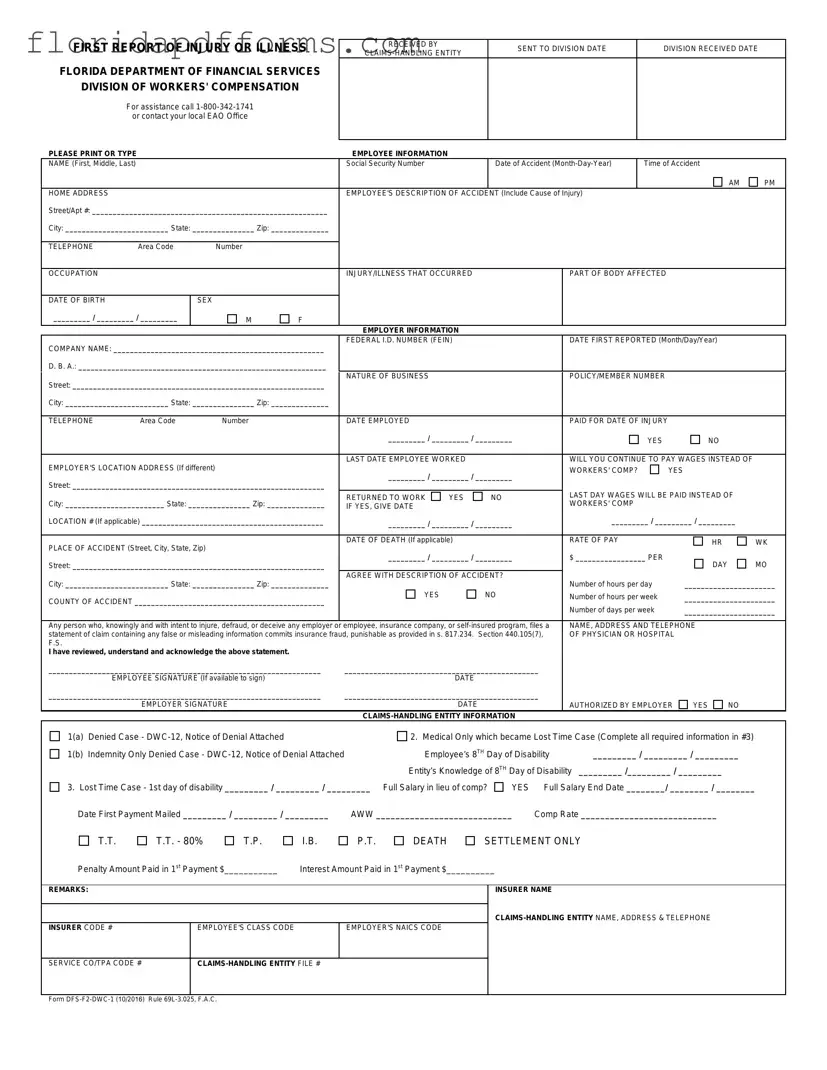
The First Report of Injury form, a crucial document in Florida’s workers' compensation system, serves as the initial notification of an employee's work-related injury or illness. This form is designed to collect essential information about the incident, including the employee's details, the nature of the injury, and specifics regarding the employer. Key elements include the employee's name, Social Security number, date and time of the accident, and a description of how the injury occurred. Employers must also provide their company name, federal ID number, and details about the business operations. The form requires confirmation of the employee’s employment status and whether wages will continue during the claims process. Additionally, it captures the location of the accident and any pertinent medical information, ensuring that all relevant parties have a clear understanding of the circumstances surrounding the incident. The completion of this form is not merely a procedural step; it is a vital part of ensuring that injured workers receive the benefits and support they need in a timely manner. By accurately filling out the First Report of Injury form, both employees and employers can navigate the complexities of the workers' compensation system more effectively.
When filing a First Report of Injury in Florida, several additional forms and documents may be required to ensure a comprehensive approach to the claim. Each of these documents serves a specific purpose and helps facilitate the processing of the injury claim.
Understanding these forms and their purposes can help streamline the claims process and ensure that all necessary information is provided. This can lead to a more efficient resolution of the injury claim, ultimately benefiting the injured employee.
The OSHA 300 Log is a document used by employers to record work-related injuries and illnesses. Similar to the First Report of Injury Florida form, it captures essential details about the incident, including the date, type of injury, and affected body parts. The OSHA 300 Log serves as a summary of all reported cases, making it easier for employers to track incidents over time. Both documents aim to ensure workplace safety by documenting injuries and promoting transparency in reporting.
The Employee Incident Report is another document that resembles the First Report of Injury Florida form. This report is typically filled out by employees immediately after an accident occurs. It includes information about the employee, the nature of the incident, and witness accounts. Like the First Report of Injury, the Employee Incident Report focuses on gathering accurate details to facilitate investigations and claims processing, ensuring that all relevant facts are documented promptly.
The Workers' Compensation Claim Form is directly related to the First Report of Injury Florida form. This form is submitted to initiate a claim for workers' compensation benefits. It requires similar information, such as the employee's details, accident description, and employer information. Both documents are essential for processing claims and ensuring that employees receive the benefits they are entitled to after a work-related injury.
The Accident Investigation Report is another document that shares similarities with the First Report of Injury Florida form. This report is created to analyze the causes of an accident and recommend safety improvements. It includes details about the incident, witnesses, and the conditions at the time of the accident. While the First Report focuses on reporting the injury, the Accident Investigation Report aims to prevent future occurrences by identifying hazards and implementing corrective actions.
The State Workers' Compensation Board Form is also comparable to the First Report of Injury Florida form. This form is used to report injuries to the state’s workers' compensation board. It collects similar information about the employee, the accident, and the employer. Both documents help ensure compliance with state regulations and facilitate the processing of claims for injured workers.
The Return to Work form is another relevant document. It is used when an employee is ready to resume work after an injury. This form often references the details provided in the First Report of Injury, ensuring that the employer is aware of any restrictions or accommodations needed. Both documents play a crucial role in managing an employee's recovery and reintegration into the workplace.
The Medical Authorization Form is similar in that it allows the employer to obtain medical records related to an employee's injury. This form is crucial for verifying the details of the injury and ensuring that the appropriate care is being provided. Like the First Report of Injury, it emphasizes the importance of accurate and timely information to support claims and treatment plans.
The Claim for Compensation form, often required in various states, is also akin to the First Report of Injury Florida form. This document is used to formally request compensation for lost wages and medical expenses resulting from a work-related injury. Both forms require detailed information about the incident and the employee’s condition, facilitating the claims process and ensuring that employees receive the support they need.
The Final Report of Injury is another document that parallels the First Report of Injury Florida form. This report is typically completed at the conclusion of a claim, summarizing the injury, treatment, and any compensation awarded. While the First Report initiates the claims process, the Final Report provides a comprehensive overview of the entire case, ensuring that all relevant details are documented and accessible for future reference.
Lastly, the Employer's Report of Injury is similar to the First Report of Injury Florida form. This document is filled out by the employer to report an employee's injury to the insurance company. It includes information about the employee, the accident, and any actions taken post-incident. Both reports are vital for ensuring that all parties are informed and that the claims process can move forward efficiently.
What is the First Report of Injury form?
The First Report of Injury form is a crucial document used in Florida to report workplace injuries or illnesses. It is required by the Florida Department of Financial Services, specifically within the Division of Workers' Compensation. This form serves as the initial notification to the employer and the state about an employee's work-related injury or illness, providing essential details necessary for processing workers' compensation claims.
Who needs to fill out the form?
The form must be filled out by the employer or their representative when an employee sustains an injury or illness while performing work-related duties. In some cases, the employee may also provide input, especially regarding their description of the accident. Accurate and complete information is vital to ensure a smooth claims process.
What information is required on the form?
The form requires various details, including:
How does the form impact workers' compensation claims?
The First Report of Injury form is a foundational document for initiating a workers' compensation claim. It triggers the claims process, allowing the insurance company to assess the situation and determine eligibility for benefits. Timely submission of this form can significantly affect the speed and outcome of the claim.
What happens if the form is not submitted on time?
Failure to submit the First Report of Injury form within the required time frame may result in delays in processing the claim. Additionally, it could lead to complications in securing benefits for the injured employee. Employers are encouraged to file the report as soon as possible after an incident occurs to avoid potential issues.
Is there a specific format for filling out the form?
Yes, the form must be completed in a clear and legible manner. It is recommended to print or type the information to ensure accuracy. Each section of the form should be filled out completely to provide all necessary details. Incomplete forms may lead to delays or rejections.
Can the form be submitted electronically?
Yes, many employers and claims-handling entities have the option to submit the First Report of Injury form electronically. However, it is essential to check with the specific workers' compensation insurance provider for their submission guidelines. Electronic submission can expedite the claims process.
What should be done after submitting the form?
After submitting the First Report of Injury form, it is advisable to keep a copy for your records. Employers should also follow up with their insurance provider to ensure the form was received and is being processed. Monitoring the claim's progress is important to address any potential issues promptly.
Where can I get assistance with the form?
For assistance with completing the First Report of Injury form, individuals can contact the Florida Department of Financial Services at 1-800-342-1741. Additionally, local Employee Assistance Offices (EAO) can provide guidance. It is beneficial to seek help if there are any uncertainties regarding the form's requirements or the claims process.
Job Applications - Input dates of attendance for all educational institutions attended.
Sf-95 - This form helps protect the privacy of employees eligible for personnel information exemption.
Motion to Travel While on Probation - Individuals should describe how they spent their free time in the past month.
FIRST REPORT OF INJURY OR ILLNESS
FLORIDA DEPARTMENT OF FINANCIAL SERVICES
DIVISION OF WORKERS' COMPENSATION
For assistance call
PLEASE PRINT OR TYPE
RECEIVED BY |
SENT TO DIVISION DATE |
DIVISION RECEIVED DATE |
|
|
|
||
|
|
|
EMPLOYEE INFORMATION
NAME (First, Middle, Last) |
|
|
|
Social Security Number |
|
|
Date of Accident |
|
Time of Accident |
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
AM |
PM |
HOME ADDRESS |
|
|
|
EMPLOYEE'S DESCRIPTION OF ACCIDENT (Include Cause of Injury) |
|
|
|
|
|||||
Street/Apt #: _________________________________________________________ |
|
|
|
|
|
|
|
|
|
|
|||
City: _________________________ State: _______________ Zip: ______________ |
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
TELEPHONE |
Area Code |
Number |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
OCCUPATION |
|
|
|
INJURY/ILLNESS THAT OCCURRED |
|
|
PART OF BODY AFFECTED |
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DATE OF BIRTH |
|
SEX |
|
|
|
|
|
|
|
|
|
|
|
_________ / _________ / _________ |
M |
F |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
EMPLOYER INFORMATION |
|
|
|
|
|
|
|
|
|
COMPANY NAME: ___________________________________________________ |
FEDERAL I.D. NUMBER (FEIN) |
|
|
DATE FIRST REPORTED (Month/Day/Year) |
|
||||||||
|
|
|
|
|
|
|
|
|
|
||||
D. B. A.: ____________________________________________________________ |
|
|
|
|
|
|
|
|
|
|
|||
Street: _____________________________________________________________ |
NATURE OF BUSINESS |
|
|
|
POLICY/MEMBER NUMBER |
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
||||
City: _________________________ State: _______________ Zip: ______________ |
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
||
TELEPHONE |
Area Code |
Number |
|
DATE EMPLOYED |
|
|
|
PAID FOR DATE OF INJURY |
|
|
|
||
|
|
|
|
_________ / _________ / _________ |
|
|
YES |
|
NO |
|
|||
|
|
|
|
|
|
|
|
|
|
||||
EMPLOYER'S LOCATION ADDRESS (If different) |
|
LAST DATE EMPLOYEE WORKED |
|
|
WILL YOU CONTINUE TO PAY WAGES INSTEAD OF |
|
|||||||
|
_________ / _________ / _________ |
WORKERS' COMP? |
|
YES |
|
||||||||
|
|
|
|
|
|
||||||||
Street: _____________________________________________________________ |
|
|
|
|
|
|
|||||||
|
|
|
|
LAST DAY WAGES WILL BE PAID INSTEAD OF |
|
||||||||
|
|
|
|
RETURNED TO WORK |
YES |
|
NO |
|
|||||
City: ________________________ State: _______________ Zip: ______________ |
|
WORKERS' COMP |
|
|
|
|
|||||||
IF YES, GIVE DATE |
|
|
|
|
|
|
|
||||||
LOCATION # (If applicable) ____________________________________________ |
_________ / _________ / _________ |
_________ / _________ / _________ |
|
||||||||||
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
RATE OF PAY |
|
|
|
|
||
PLACE OF ACCIDENT (Street, City, State, Zip) |
|
DATE OF DEATH (If applicable) |
|
|
|
|
HR |
WK |
|||||
|
|
|
|
|
|
|
|
|
|||||
|
_________ / _________ / _________ |
$ _________________ PER |
|
|
|
||||||||
Street: _____________________________________________________________ |
|
DAY |
MO |
||||||||||
|
|
|
|
|
|
|
|
||||||
City: _________________________ State: _______________ Zip: ______________ |
AGREE WITH DESCRIPTION OF ACCIDENT? |
Number of hours per day |
______________________ |
||||||||||
|
|
|
|
||||||||||
COUNTY OF ACCIDENT ______________________________________________ |
YES |
|
NO |
Number of hours per week |
______________________ |
||||||||
|
|
|
|
Number of days per week |
______________________ |
||||||||
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|||||||||
Any person who, knowingly and with intent to injure, defraud, or deceive any employer or |
employee, insurance company, or |
NAME, ADDRESS AND TELEPHONE |
|
||||||||||
statement of claim containing any false or misleading information commits insurance fraud, punishable as provided in s. 817.234. Section 440.105(7), |
OF PHYSICIAN OR HOSPITAL |
|
|||||||||||
F.S. |
|
|
|
|
|
|
|
|
|
|
|
|
|
I have reviewed, understand and acknowledge the above statement.
__________________________________________________________________ |
_______________________________________________ |
|
|
|
|||
|
EMPLOYEE SIGNATURE (If available to sign) |
DATE |
|
|
|
|
|
__________________________________________________________________ |
_______________________________________________ |
|
|
|
|||
|
EMPLOYER SIGNATURE |
DATE |
|
AUTHORIZED BY EMPLOYER |
YES |
NO |
|
|
|
|
|
|
|
||
1(a) |
Denied Case - |
2. Medical Only which became Lost Time Case (Complete all required information in #3) |
|||||
1(b) |
Indemnity Only Denied Case - |
Employee’s 8TH Day of Disability |
_________ / _________ / _________ |
||||
|
|
Entity’s Knowledge of 8TH Day of Disability |
_________ /_________ / _________ |
|
|||
3. Lost Time Case - 1st day of disability _________ / _________ / _________ Full Salary in lieu of comp? |
YES |
Full Salary End Date ________/ ________ / ________ |
|||||
Date First Payment Mailed _________ / _________ / _________ |
AWW ____________________________ |
Comp Rate ____________________________ |
|
||||
T.T.
T.T. - 80%
T.P.
I.B.
P.T.
DEATH
SETTLEMENT ONLY
Penalty Amount Paid in 1st Payment $___________ |
Interest Amount Paid in 1st Payment $__________ |
REMARKS:
INSURER CODE # |
EMPLOYEE'S CLASS CODE |
EMPLOYER'S NAICS CODE |
|
|
|
INSURER NAME
SERVICE CO/TPA CODE #
Form
The collection of the social security number on this form is specifically authorized by Section 440.185(2), Florida Statutes. The social security number will be used as a unique identifier in Division of Workers' Compensation database systems for individuals who have claimed benefits under Chapter 440, Florida Statutes. It will also be used to identify information and documents in those database systems regarding individuals who have claimed benefits under Chapter 440, Florida Statutes, for internal agency tracking purposes and for purposes of responding to both public records requests and subpoenas that require production of specified documents. The social security number may also be used for any other purpose specifically required or authorized by state or federal law.
When filling out the First Report of Injury form in Florida, attention to detail is crucial. Here are four important dos and don'ts to keep in mind: